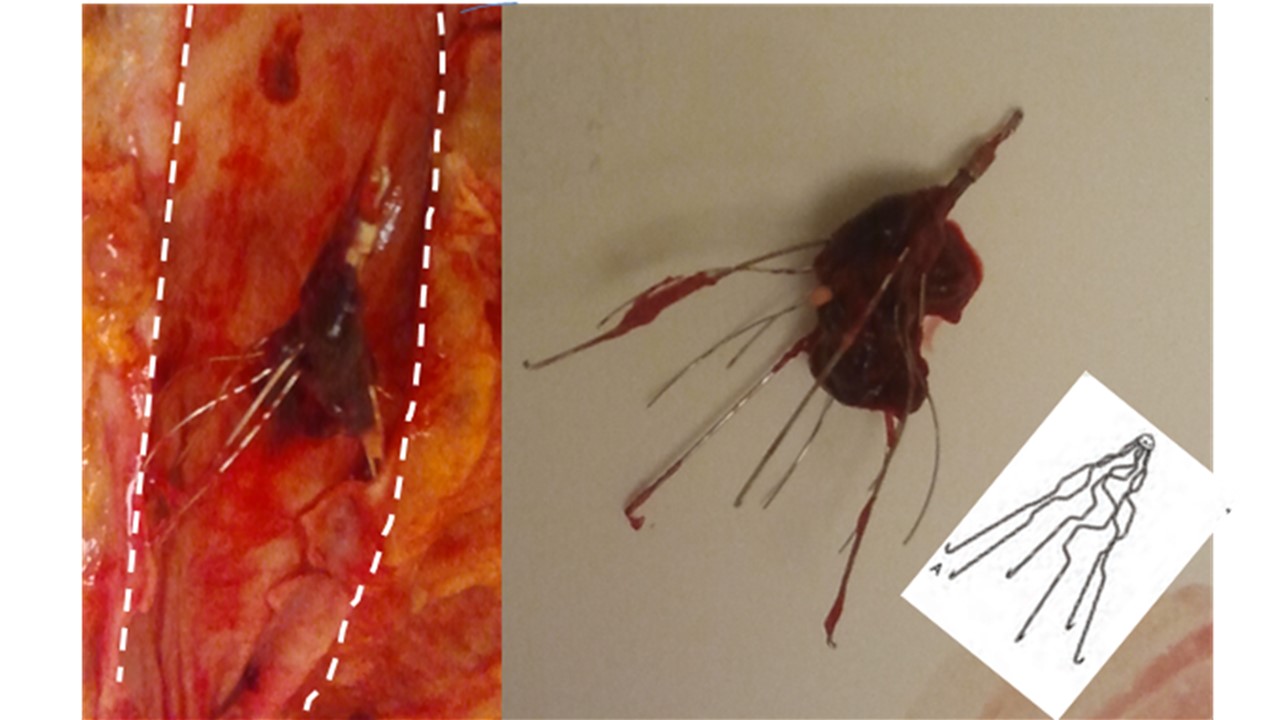
 What is shown? The top photo shows the pancreas split down the middle (horizontally). To the left is the tumor. Next to the tumor is a circle. This is a tube cut across. It is the common bile duct (the tube that drains bile from the liver). The tube is abnormal. It’s too big (dilated). It is roughly twice as big as it should be normally. To the right is the spleen (the red organ taking up about a third of the image). Below, the photo is illustrated. The split down the middle of the pancreas is shown with a dashed red line. The tumor is outlined in black. Two red arrows highlight the common bile duct. The spleen is labelled.
What is shown? The top photo shows the pancreas split down the middle (horizontally). To the left is the tumor. Next to the tumor is a circle. This is a tube cut across. It is the common bile duct (the tube that drains bile from the liver). The tube is abnormal. It’s too big (dilated). It is roughly twice as big as it should be normally. To the right is the spleen (the red organ taking up about a third of the image). Below, the photo is illustrated. The split down the middle of the pancreas is shown with a dashed red line. The tumor is outlined in black. Two red arrows highlight the common bile duct. The spleen is labelled.
What was the story here? This case was from an autopsy of a man in his 50’s who had cancer of “undiagnosed primary.” This means that he had cancer in his body but no one knew where the cancer started. Specifically, he had cancer that had spread to his lymph nodes. He had a biopsy of one of these lymph nodes. Testing of the lymph node tissue showed that one possibility was that the tumor started in the pancreas. But x-ray studies did not report a mass in the pancreas. The x-rays showed the common bile duct was dilated, but no mass in the pancreas. The pancreas was never biopsied.
Why did the family request an autopsy? The family wanted to finally find out where the tumor came from. They were angry that no diagnosis had been made.
Why was the diagnosis not made here? In this particular case, the tumor did not increase the size of the pancreas very much and, as mentioned, could not be seen on x-ray. Some pancreatic tumors are not visible on x-ray. These tumors are called “isodense.” “Iso” means “same.” So these tumors have the same density as normal tissue. Approximately 10% of pancreatic tumors are isodense. This means they cannot be distinguished in x-ray appearance from normal pancreatic tissue.
On the other hand, a tell tale sign of a pancreatic cancer is that it can pinch off the tip of the common bile duct and cause the rest of the duct to balloon out. This happened here. But the finding was not considered in thinking about the possibility of a pancreatic tumor.
Lastly, the lymph node that was positive for cancer was in a unique place in the body. It was above the left collar bone. A lymph node here is called a “Virchow’s node.” It is a tip off that the tumor could come from the pancreas.
So overall, there were three tell-tale signs to consider there might be a tumor in the pancreas: the studies on the lymph node, the location of the lymph node, and the ballooned (dilated) common bile duct. But because no mass was seen on x-ray, pancreatic cancer was not considered. There was no consideration the tumor was hidden on x-ray because it was isodense; and, again, no biopsy. This was a missed diagnosis.
How did the autopsy help? The autopsy provided closure for the family because it answered an important question they wanted and needed to know: where did the tumor come from? And it gave them a context for understanding the factors that went into the missed diagnosis.