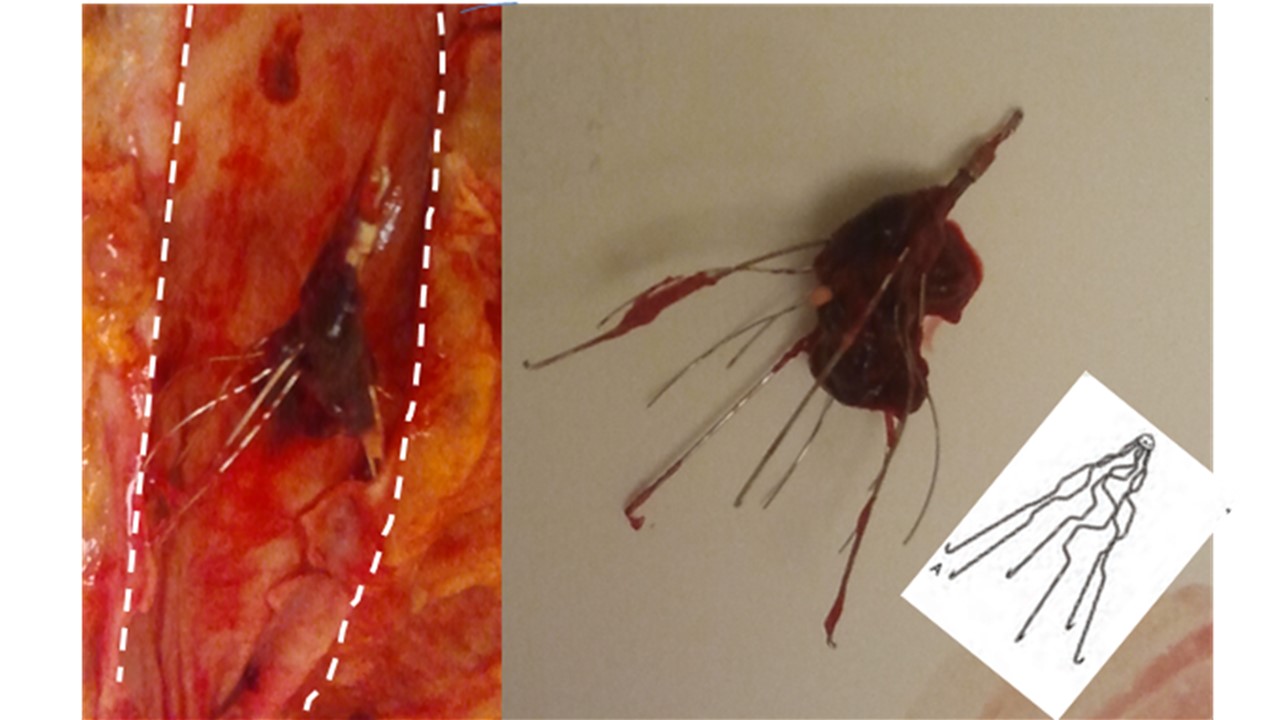
What is shown? Shown (right photo) is a piece of metal wiring with blood clot trapped in it. The device is called a Greenfield filter. It’s about two inches long altogether. The left picture shows the device where it was found – in the inferior vena cava (dashed lines). The inferior vena has been opened up along its length. The diagrammatic insert shows the filter without clot attached.
What is a Greenfield filter? A Greenfield filter is a device inserted into the inferior vena cava (the large vein returning blood to the heart). The filter traps clot that might travel up from the legs in some patients. It is inserted through the groin and threaded up the inferior vena cava to rest there.
How does the filter stay put? Little hooks at the ends of the wires keep it in place inside the vein. This keeps it from traveling up the vein closer to the heart
How does the filter help the patient? By trapping clots that travel in the blood stream up from the legs, the filter prevents them from traveling any farther. Specifically, the filter prevents them from reaching the lungs. The Greenfield filter saves lives.
Who gets a Greenfield filter? Patients with clots in their legs (deep venous thromboses – DVT’s) get a Greenfield filter.
What was the story here? This was a 32 year old man with cancer (lymphoma), DVT, and many infections. He spent the six months leading up to his death in the hospital.
Why did the family request and autopsy? The family was looking for closure and peace of mind. They were also concerned about the quality of care and the possibility of missed diagnoses. The family was dedicated and committed and had one member or another stay with him at all times. Their style was centered on control with extensive documentation and detailed note-taking of any medical information or conversations that came their way. Behind all this were deep feelings of grief over the loss of a son and brother.
How did the autopsy help? In the setting of deep grief, it was important to make use of any and all information from the autopsy to provide both a clear picture of the quality of care and the patient’s experience prior to death. The finding of a Greenfield filter with entrapped clot indicated the following:
Filter placement. The presence of the filter itself reflected appropriate clinical judgment and excellent quality care on the part of the providers. It is standard of care to place the filter, which is what this patient had. For a family with concerns about treatment, it was then helpful to objectively show that at least in one area (management of deep venous thrombosis), care had been appropriate. This then, could help the family feel a bit less angry about some of their concerns. It was not clear what, if anything, had already been discussed with the family about the filter’s placement. Its finding at autopsy presented another opportunity to review the clinical course.
Trapped clot. The presence of trapped clot indicated a disaster avoided. The amount of clot was significant. Without the filter the clot would have, without a doubt, traveled up the blood stream to the lungs and possibly caused the patient’s death, if not severe illness.
Conclusion. Therefore, for during a life cut short, when days and weeks had become precious to the patient and to the family, it was clear that the medical care had bought some time in this world for this patient. This was an important thing to share with a family dealing with loss; and a benefit of the autopsy.
[button label=”Latest News, Events and Articles” url=”/” target=”_blank” color=”#f05134″]